结核与肺部疾病杂志 ›› 2025, Vol. 6 ›› Issue (3): 316-322.doi: 10.19983/j.issn.2096-8493.20250069
侯坤1,2, 伍劲屹2, 王晓君3, 彭鹏2( )
)
Hou Kun1,2, Wu Jinyi2, Wang Xiaojun3, Peng Peng2()
摘要:
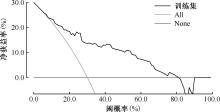
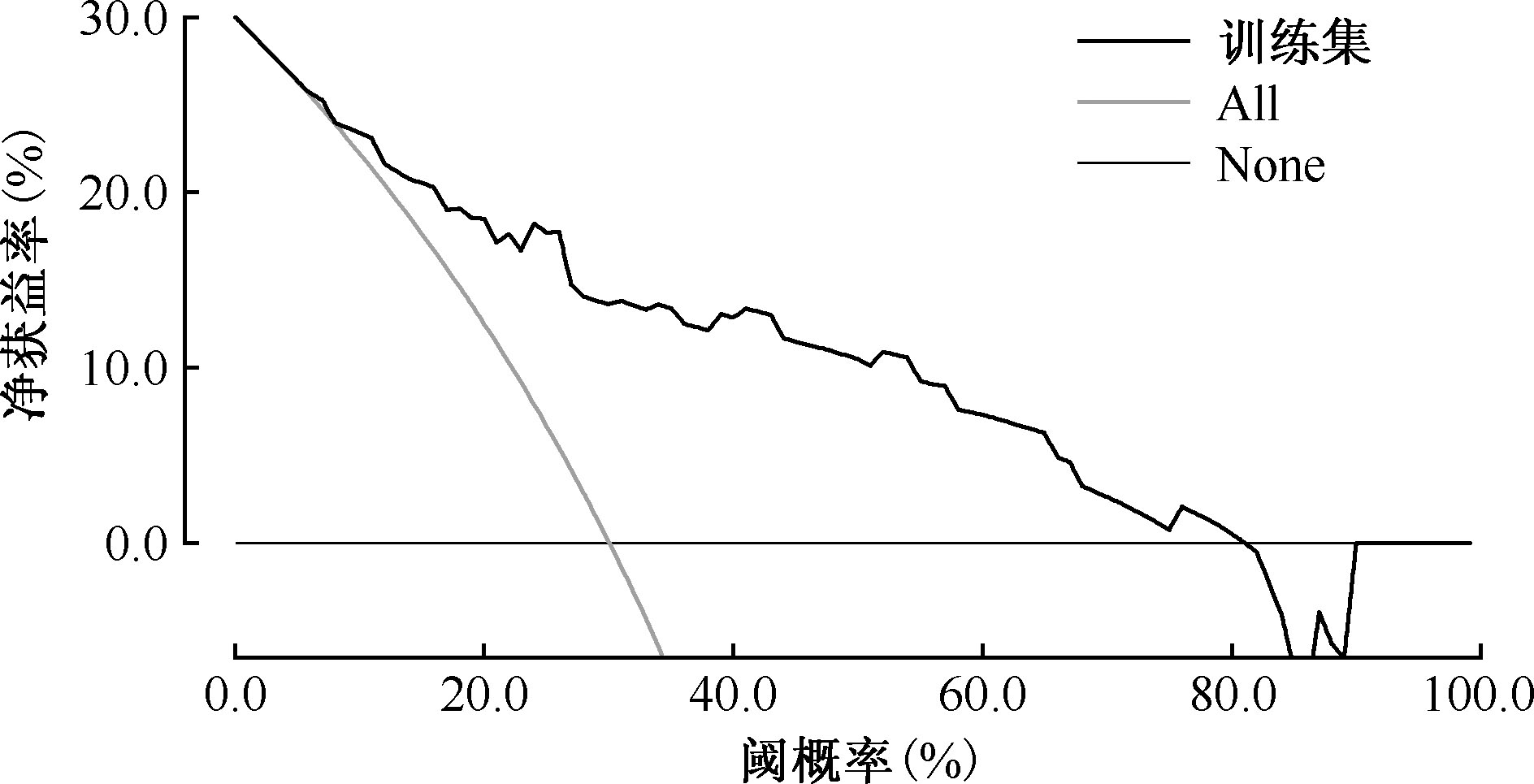
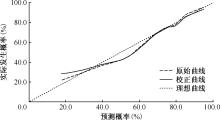
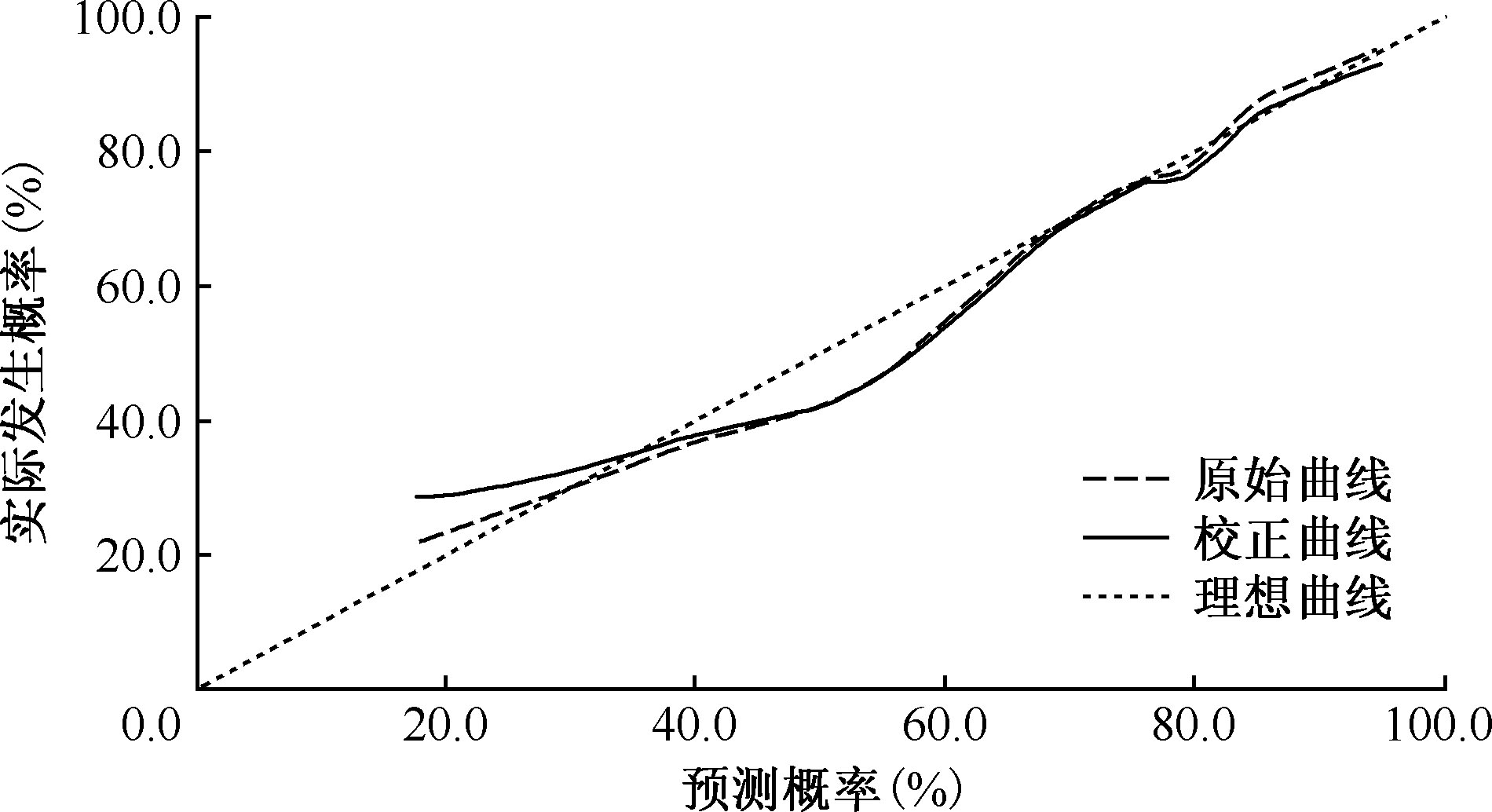
目的:了解武汉市第四医院肺结核延迟诊断现状,分析诊断延迟影响因素并构建风险预测模型,为优化肺结核防治措施提供依据。方法:参照入组标准,从中国疾病预防控制信息系统中选取2020年1月1日至2022年12月31日武汉市上报且在报卡前6个月内在武汉市第四医院有就诊记录的125例肺结核患者为研究对象,从医院病案信息系统中收集患者的相关人口学特征和临床资料。采用描述性、单因素及多因素logistic回归模型分析诊断延迟影响因素,并构建风险预测模型;使用受试者工作特征曲线下面积(AUC)、决策曲线分析(DCA)和校准曲线(CC)评估模型性能。结果:125例患者的报卡时间间隔中位数(四分位数)为49(13,110)d,诊断延迟率为74.40%(93/125),开具影像学或结核病相关检测者66例(52.80%)。本院报卡者34例(27.20%),报卡时间间隔为10(5,81)d,诊断率延迟为44.12%(15/34),开具影像学或结核病相关检测的比例为100.00%(34/34);外院报卡者91例(72.80%),报卡时间间隔为58(23,114)d,诊断延迟率为85.71%(78/91),开具影像学或结核病相关检测的比例为35.16%(32/91);本院与外院在报卡时间间隔、开具影像学或结核病相关检测比例和诊断延迟率的差异均有统计学意义(Z=-3.199,P=0.001;χ2=41.750,P=0.001;χ2=22.486,P=0.001);呼吸内科诊断延迟率[33.33%(7/21)]明显低于其他科室[82.69%(86/104)],差异有统计学意义(χ2=22.349,P<0.001)。Logistic多因素分析结果显示,首诊科室为呼吸内科及本院就诊时开具影像学或结核病相关检测均是诊断延迟的保护因素(OR=0.182,95%CI:0.055~0.597;OR=0.196, 95%CI:0.065~0.588)。肺结核诊断延迟风险预测模型训练集的AUC值为0.820,内部验证集的AUC值为0.833,DCA结果显示该模型在6%~80%阈概率时具有临床实用性,CC曲线显示预测值与真实值之间具有良好的一致性。结论:本院肺结核诊断延迟率较高,非呼吸内科首诊和本院就诊时未开具影像学或结核病相关检测均是影响患者发生诊断延迟的独立危险因素。构建的风险预测模型具有较好的预测性能。建议加强结核病首诊工作,通过系统化、长期化的培训提升综合医院医生,尤其是非呼吸专科医生对肺结核的识别能力,并提高院内报卡及时性。
中图分类号:
 京公安网备11010202008787号
ip访问总数: ip当日访问总数: 当前在线人数:
京公安网备11010202008787号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可