结核病与肺部健康杂志 ›› 2018, Vol. 7 ›› Issue (4): 305-310.doi: 10.3969/j.issn.2095-3755.2018.04.016
冯勇,梁洪斌,丁卫忠( )
)
Yong FENG,Hong-bin LIANG,Wei-zhong DING()
摘要:
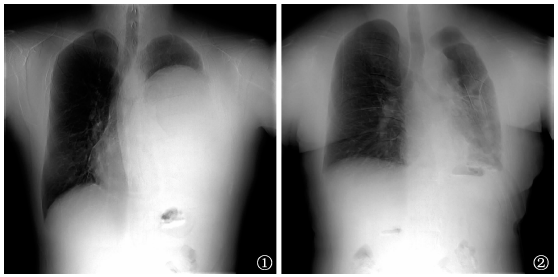
目的 探讨慢性巨大结核性脓胸的手术治疗方式。方法 收集2015—2017年沈阳市胸科医院行手术切除术并经术后病理证实为结核性脓胸、且术前X线胸部摄影(简称“胸片”)显示脓腔占据患侧胸腔50%以上者36例,包括20例巨大包裹性脓胸、16例全脓胸。分析胸膜纤维板剥脱术、胸膜肺切除术、胸廓成形术3种术式对不同患者的治疗效果。结果 36例患者均完整切除病变部位。26例患者行胸膜纤维板剥脱术,包括20例巨大包裹性脓胸、6例全脓胸,其中10例巨大包裹性脓胸患者行肺脏层胸膜纤维板剥除后,肺膨胀欠佳,遗留较小残腔,保留了壁层胸膜纤维板;术后经闭式引流2~8周左右,并配合负压吸引,肺膨胀良好,残腔消失,痊愈出院。7例全脓胸并发毁损肺患者行胸膜肺切除术,其中2例因肺完全不能膨胀,行胸膜纤维板剥脱术+全肺切除术;5例因并发单个肺叶内结核病变较重,但健侧肺脏层胸膜破损不重且膨胀良好,行胸膜纤维板剥脱术+肺叶切除术;术后均给予1~3d机械通气及6~9个月规范抗结核药物治疗,临床治愈。3例全脓胸患者行胸廓成形术,其中1例并发支气管胸膜瘘患者直接行胸廓成形术;另2例因肺内结核病灶相对稳定,剥除肺脏层胸膜纤维板、保留壁层纤维板后肺仍膨胀不良,遗留有较大残腔,直接行胸膜纤维板剥脱术+局限性胸廓成形术;术后切口加压包扎,3周后痊愈出院。26例行胸膜纤维板剥脱术患者中发生内出血1例,7例胸膜肺切除患者中发生急性呼吸衰竭1例,3例胸廓成形术患者中发生切口愈合不良1例。结论 胸膜纤维板剥脱术是结核性脓胸的首选治疗方式,在严格把握手术适应证的基础上,3种术式对于不同患者治疗均安全有效。
 京公安网备11010202008787号
ip访问总数: ip当日访问总数: 当前在线人数:
京公安网备11010202008787号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可