
Journal of Tuberculosis and Lung Disease ›› 2025, Vol. 6 ›› Issue (5): 516-524.doi: 10.19983/j.issn.2096-8493.20250065
• Original Articles • Previous Articles Next Articles
Xu Siyun1,2, Lu Nihong1( )
)
Received:2025-04-17
Online:2025-10-20
Published:2025-10-15
Contact:
Lu Nihong
E-mail:602157606@qq.com
Supported by:CLC Number:
Xu Siyun, Lu Nihong. The value of serum inflammatory index combined with chest CT in differential diagnosis of benign and malignant pulmonary nodules[J]. Journal of Tuberculosis and Lung Disease , 2025, 6(5): 516-524. doi: 10.19983/j.issn.2096-8493.20250065
Add to citation manager EndNote|Ris|BibTeX
URL: https://www.jtbld.cn/EN/10.19983/j.issn.2096-8493.20250065
| 特征 | 良性组(126例) | 恶性组(127例) | 统计检验值 | P值 |
|---|---|---|---|---|
| 年龄(岁, | 58.51±10.44 | 61.09±11.97 | t=1.831 | 0.068 |
| 性别[例,构成比(%)] | χ2=0.244 | 0.621 | ||
| 男性 | 87(69.0) | 84(66.1) | ||
| 女性 | 39(31.0) | 43(33.9) | ||
| 结节数量[例,构成比(%)] | χ2=28.389 | <0.001 | ||
| 孤立性 | 18(14.3) | 57(44.9) | ||
| ≥2个 | 108(85.7) | 70(55.1) | ||
| 结节直径[例,构成比(%)] | χ2=55.453 | <0.001 | ||
| 5~8mm | 98(77.8) | 47(37.0) | ||
| 8~15mm | 16(12.7) | 14(11.0) | ||
| 15~30mm | 12(9.5) | 66(52.0) | ||
| 分叶征[例,构成比(%)] | χ2=36.969 | <0.001 | ||
| 是 | 6(4.8) | 45(35.4) | ||
| 否 | 120(95.2) | 82(64.6) | ||
| 毛刺征[例,构成比(%)] | χ2=35.620 | <0.001 | ||
| 是 | 6(4.8) | 44(34.6) | ||
| 否 | 120(95.2) | 83(65.4) | ||
| 血管束集征[例,构成比(%)] | χ2=5.772 | 0.016 | ||
| 是 | 10(7.9) | 23(18.1) | ||
| 否 | 116(92.1) | 104(81.9) | ||
| CT值(HU, | -306.41±248.614 | -359.51±154.73 | t=2.038 | 0.043 |
| 检测指标 | 良性组 (126例) | 恶性组(127例) | Z值 | P值 | ||
|---|---|---|---|---|---|---|
| 腺癌(87例) | 鳞癌(25例) | 小细胞癌(15例) | ||||
| NLR[M(Q1,Q3)] | 2.50 (1.86,3.56) | 2.59 (1.90,4.73) | 4.04 (3.17,7.02)ab | 3.73 (2.31,6.25) | 19.979 | <0.001 |
| LMR[M(Q1,Q3)] | 3.34 (2.54,4.58) | 3.06 (2.10,4.42)a | 2.27 (1.28,3.14)ab | 2.49 (1.33,2.93) | 19.259 | <0.001 |
| PLR[M(Q1,Q3)] | 165.52 (125.87,206.43) | 165.58 (115.34,238.68) | 227.52 (147.18,368.42) | 150.89 (89.23,293.87) | 6.166 | 0.104 |
| SII[×109g/L,M(Q1,Q3)] | 582.06 (392.98,854.01) | 640.19 (363.59,1155.42) | 1390.96 (889.04,2486.67)ab | 711.47 (414.28,1384.94) | 18.224 | <0.001 |
| IL-5[pg/ml,M(Q1,Q3)] | 2.68 (1.93,4.37) | 2.93 (2.03,4.04) | 5.46 (2.57,10.13)ab | 2.20 (0.88,3.30)c | 15.235 | 0.002 |
| IFN-α[pg/ml,M(Q1,Q3)] | 2.81 (1.84,4.04) | 2.52 (1.52,4.12) | 2.67 (2.22,3.15) | 2.09 (1.48,2.65) | 4.386 | 0.223 |
| IL-2[pg/ml,M(Q1,Q3)] | 6.20 (2.67,21.61) | 4.68 (2.21,8.09)a | 3.65 (2.15,4.87)a | 9.25 (4.69,16.81)c | 19.389 | <0.001 |
| IL-6[pg/ml,M(Q1,Q3)] | 3.82 (1.46,9.08) | 9.82 (4.46,18.02)a | 20.33 (6.04,34.15)a | 18.92 (11.94,72.95)a | 41.903 | <0.001 |
| IL-1β[pg/ml,M(Q1,Q3)] | 5.48 (3.07,12.39) | 9.72 (3.74,16.95) | 6.76 (3.90,8.30) | 23.28 (16.16,30.40)abc | 21.607 | <0.001 |
| IL-10[pg/ml,M(Q1,Q3)] | 3.30 (2.44,4.88) | 2.85 (1.96,4.53) | 1.86 (1.67,2.26)ab | 4.86 (3.62,6.07)bc | 34.980 | <0.001 |
| IFN-γ[pg/ml,M(Q1,Q3)] | 11.05 (5.48,17.78) | 10.19 (5.69,19.60) | 6.87 (5.31,7.60)ab | 9.27 (4.43,13.01) | 15.529 | 0.001 |
| IL-8[pg/ml,M(Q1,Q3)] | 3.39 (1.73,9.41) | 11.42 (4.41,19.77)a | 22.58 (8.55,29.34)a | 2.73 (1.69,4.51)bc | 31.181 | <0.001 |
| IL-17[pg/ml,M(Q1,Q3)] | 4.13 (2.75,10.11) | 2.90 (1.56,4.35)a | 4.45 (2.61,6.13) | 7.12 (3.65,10.62)b | 29.143 | <0.001 |
| IL-12P70[pg/ml,M(Q1,Q3)] | 2.01 (1.65,2.21) | 2.00 (1.44,2.30) | 1.53 (1.06,2.04) | 2.05 (1.26,2.91) | 4.878 | 0.197 |
| TNF-α[pg/ml,M(Q1,Q3)] | 2.64 (1.72,3.99) | 4.00 (2.47,6.63)a | 2.33 (1.87,2.67)b | 2.32 (2.19,2.55)ab | 32.271 | <0.001 |
| CRP[mg/L,M(Q1,Q3)] | 7.95 (1.64,28.03) | 11.09 (2.77,24.43) | 29.41 (11.46,67.74)a | 14.06 (8.60,43.37) | 12.121 | 0.007 |
| PCT[ng/ml,M(Q1,Q3)] | 0.09 (0.04,0.16) | 1.26 (0.45,2.41)a | 0.33 (0.10,0.98)a | 0.10 (0.06,0.12)b | 102.644 | <0.001 |
| SAA[mg/L,M(Q1,Q3)] | 24.15 (3.40,101.77) | 236.26 (75.62,322.80)a | 144.39 (36.70,254.35)a | 112.78 (73.08,129.19) | 61.595 | <0.001 |
| 自变量 | 赋值 |
|---|---|
| 结节数量 | 0=孤立性;1=结节数量≥2个 |
| 结节直径 | 1=5~8mm;2=8~15mm;3=15~30mm |
| 毛刺征 | 1=是;0=否 |
| 分叶征 | 1=是;0=否 |
| 血管集束征 | 1=是;0=否 |
| 影响因素 | β值 | s | Wald χ2值 | OR值 | 95%CI值 | P值 |
|---|---|---|---|---|---|---|
| 结节直径8~15mm | 2.329 | 0.912 | 6.525 | 10.268 | 1.719~61.321 | 0.011 |
| 结节直径15~30mm | 4.081 | 0.852 | 22.967 | 59.194 | 11.155~314.124 | <0.001 |
| 毛刺征 | 3.310 | 0.994 | 11.085 | 27.373 | 3.901~192.055 | 0.001 |
| LMR | -0.757 | 0.259 | 8.552 | 0.469 | 0.282~0.779 | 0.003 |
| IL-5 | 0.443 | 0.157 | 7.962 | 1.557 | 1.145~2.118 | 0.005 |
| Il-2 | -0.185 | 0.054 | 11.830 | 0.831 | 0.748~0.924 | 0.001 |
| SAA | 0.965 | 0.318 | 9.201 | 2.625 | 1.407~4.897 | 0.002 |
| PCT | 0.567 | 0.180 | 9.970 | 1.763 | 1.240~2.507 | 0.002 |
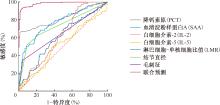
| 检测项目 | AUC值 | AUC的95%CI值 | P值 | 敏感度 | 特异度 | 正确指数 | 截断值 |
|---|---|---|---|---|---|---|---|
| 结节直径 | 0.732 | 0.669~0.795 | <0.001 | 0.52 | 0.90 | 0.905 | 2.50 |
| 毛刺征 | 0.649 | 0.581~0.717 | <0.001 | 0.36 | 0.95 | 0.952 | 0.50 |
| LMR | 0.398 | 0.532~0.672 | 0.005 | 0.50 | 0.69 | 0.193 | 3.40 |
| IL-5 | 0.516 | 0.445~0.588 | 0.037 | 0.49 | 0.63 | 0.119 | 3.16 |
| IL-2 | 0.380 | 0.311~0.450 | 0.007 | 0.33 | 0.95 | 0.286 | 14.44 |
| SAA | 0.773 | 0.715~0.830 | <0.001 | 0.69 | 0.75 | 0.439 | 102.46 |
| PCT | 0.821 | 0.767~0.874 | <0.001 | 0.67 | 0.98 | 0.653 | 0.30 |
| 联合检测 | 0.983 | 0.971~0.995 | <0.001 | 0.92 | 0.97 | 0.890 | 0.53 |

| [1] | Cao W, Qin K, Li F, et al. Comparative study of cancer profiles between 2020 and 2022 using global cancer statistics (GLOBOCAN) Comparative study of cancer profiles between J Natl Cancer Cent, 2024, 4(2):128-134. doi:10.1016/j.jncc.2024.05.001. |
| [2] | Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent, 2024, 4(1): 47-53. doi:10.1016/j.jncc.2024.01.006. |
| [3] | 中华医学会肿瘤学分会. 中华医学会肺癌临床诊疗指南(2024版). 中华医学杂志, 2024, 104(34):3175-3213. doi:10.3760/cma.j.cn112137-20240511-01092. |
| [4] | 姚俊, 宋晓. 吉西他滨和顺铂方案联合康莱特注射液治疗晚期非小细胞肺癌的临床分析. 临床和实验医学杂志, 2017, 16(12):1195-1198. doi:10.3969/j.issn.1671-4695.2017.12.018. |
| [5] | Liu ZL, Zhu WR, Zhou WC, et al. Traditional Chinese medi-cinal herbs combined with epidermal growth factor receptor tyrosine kinase inhibitor for advanced non-small cell lung cancer: a systematic review and meta-analysis. J Integr Med, 2014, 12(4):346-358. doi:10.1016/S2095-4964(14)60034-0. |
| [6] | 朱严严. 肿瘤标志物联合胸部影像学在肺癌早期诊断中的价值研究. 现代医用影像学, 2023, 32(8):1503-1505. doi:10.3969/j.issn.1006-7035.2023.08.033. |
| [7] | Jonas DE, Reuland DS, Reddy SM, et al. Screening for Lung Cancer With Low-Dose Computed Tomography: Updated Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA, 2021, 325(10):971-987. doi:10.1001/jama.2021.0377. |
| [8] | Zhou Y, Tao L, Qiu J, et al. Tumor biomarkers for diagnosis, prognosis and targeted therapy. Signal Transduct Target Ther, 2024, 9(1):132. doi:10.1038/s41392-024-01823-2. |
| [9] | 李源, 闵旭红, 王彬, 等. CT引导下经皮肺部病灶穿刺活检常见并发症影响因素与处理. 安徽医学, 2023, 44(6):697-701. doi:10.3969/j.issn.1000-0399.2023.06.017. |
| [10] | Bouras E, Karhunen V, Gill D, et al. Circulating inflammatory cytokines and risk of five cancers: a Mendelian randomization analysis. BMC Med, 2022, 20(1):3. doi:10.1186/s12916-021-02193-0. |
| [11] | Marozzi M, Parnigoni A, Negri A, et al. Inflammation, Extracellular Matrix Remodeling, and Proteostasis in Tumor Microenvironment. Int J Mol Sci, 2021, 22(15):8102. doi:10.3390/ijms22158102. |
| [12] | Lim JS, Ibaseta A, Fischer MM, et al. Intratumoural heterogeneity generated by Notch signalling promotes small-cell lung cancer. Nature, 2017, 545(7654):360-364. doi:10.1038/nature22323. |
| [13] | Xu K, Zhang C, Du T, et al. Progress of exosomes in the diagnosis and treatment of lung cancer. Biomed Pharmacother, 2021, 134:111111. doi:10.1016/j.biopha.2020.111111. |
| [14] | Walter JE, Heuvelmans MA, de Jong PA, et al. Occurrence and lung cancer probability of new solid nodules at incidence screening with low-dose CT: analysis of data from the randomi-sed, controlled NELSON trial. Lancet Oncol, 2016, 17(7):907-916. doi:10.1016/S1470-2045(16)30069-9. |
| [15] | De Koning HJ, van der Aalst CM, de Jong PA, et al. Reduced Lung-Cancer Mortality with Volume CT Screening in a Randomized Trial. N Engl J Med, 2020, 382(6):503-513. doi:10.1056/NEJMoa1911793. |
| [16] | Lancaster HL, Heuvelmans MA, Oudkerk M. Low-dose computed tomography lung cancer screening: Clinical evidence and implementation research. J Intern Med, 2022, 292(1):68-80. doi:10.1111/joim.13480. |
| [17] | Song M, Zhang Q, Song C, et al. The advanced lung cancer inflammation index is the optimal inflammatory biomarker of overall survival in patients with lung cancer. J Cachexia Sarcopenia Muscle, 2022, 13(5):2504-2514. doi:10.1002/jcsm.13032. |
| [18] | Pelosi G, Sonzogni A, Viale G. The classification of lung carcinoma: time to change the morphology-based approach?. Int J Surg Pathol, 2010, 18(3):161-172. doi:10.1177/1066896910361736. |
| [19] | Tammemagi M, Ritchie AJ, Atkar-Khattra S, et al. Predicting Malignancy Risk of Screen-Detected Lung Nodules-Mean Diameter or Volume. J Thorac Oncol, 2019, 14(2):203-211. doi:10.1016/j.jtho.2018.10.006. |
| [20] | 谢惠杰, 邹红, 吴赓, 等. 血常规炎症指标联合血清肿瘤标志物在肺癌诊断中的价值分析. 检验医学与临床, 2023, 20(6):758-763. doi:10.3969/j.issn.1672-9455.2023.06.010. |
| [21] | 汤欣. 螺旋CT引导下经皮肺穿刺活检对不同大小肺结节及良恶性诊断的效能. 影像研究与医学应用, 2024, 8(17):179-181,184. doi:10.3969/j.issn.2096-3807.2024.17.057. |
| [22] | 李婷, 黄麟洲, 张仕勇, 等. 肺部磨玻璃结节的高分辨CT征象及其评估肿瘤恶性侵袭程度的价值. 广西医学, 2024, 46(6):828-833. doi:10.11675/j.issn.0253-4304.2024.06.08. |
| [23] | 许健, 李锋, 周芳, 等. 孤立性肺结节患者MSCT征象特点及其筛查价值分析. 中国CT和MRI杂志, 2021, 19(4):57-59. doi:10.3969/j.issn.1672-5131.2021.04.019. |
| [24] | 蒋雨珂, 李长毅. 新型炎症标志物在肺癌中的应用. 现代医药卫生, 2024, 40(1):111-116,121. doi:10.3969/j.issn.1009-5519.2024.01.022. |
| [25] | Zhai B, Chen J, Wu J, et al. Predictive value of the hemoglobin, albumin, lymphocyte, and platelet (HALP) score and lymphocyte-to-monocyte ratio (LMR) in patients with non-small cell lung cancer after radical lung cancer surgery. Ann Transl Med, 2021, 9(12):976. doi:10.21037/atm-21-2120. |
| [26] | Sun H, Lee HS, Kim SH, et al. IL-2 can signal via chemokine receptors to promote regulatory T cells’ suppressive function. Cell Rep, 2023, 42(8):112996. doi:10.1016/j.celrep.2023.112996. |
| [27] | Hou Y, Xiang B, Yang Z, et al. Down-regulation of interleukin-2 predicts poor prognosis and associated with immune escape in lung adenocarcinoma. Int J Immunopathol Pharmacol, 2023, 37:3946320231202748. doi:10.1177/03946320231202748. |
| [28] | 韩翔, 张培, 王娟, 等. 肺癌组织中嗜酸细胞浸润及白细胞介素5表达的意义. 中华医学杂志, 2011, 91(14):956-960. doi:10.3760/cma.j.issn.0376-2491.2011.14.005. |
| [29] | Cremona M, Calabrò E, Randi G, et al. Elevated levels of the acute-phase serum amyloid are associated with heightened lung cancer risk. Cancer, 2010, 116(5):1326-1335. doi:10.1002/cncr.24868. |
| [30] | Sung HJ, Ahn JM, Yoon YH, et al. Identification and validation of SAA as a potential lung cancer biomarker and its involvement in metastatic pathogenesis of lung cancer. J Proteome Res, 2011, 10(3):1383-1395. doi:10.1021/pr101154j. |
| [31] | Chaftari AM, Hachem R, Reitzel R, et al. Role of Procalcitonin and Interleukin-6 in Predicting Cancer, and Its Progression Independent of Infection. PLoS One, 2015, 10(7):e0130999. doi:10.1371/journal.pone.0130999. |
| [1] | Fan Guiqin, Lyu Hong, Qu Qiuxia. Investigate the regulatory effect of Astragalus Polysaccharides on lung cancer tissue infiltrating PD-1hiCD8+T cell subsets in mice [J]. Journal of Tuberculosis and Lung Disease, 2025, 6(4): 393-400. |
| [2] | Wei Yunxia, Wang Xin, Long Xuejuan. Prognostic value of neutrophil-to-lymphocyte ratio combined with serum procalcitonin in patients with severe pulmonary tuberculosis [J]. Journal of Tuberculosis and Lung Disease, 2025, 6(3): 330-334. |
| [3] | Lin Hong, Yu Jinfeng, Zhang Shouxia, Liu Ye, Chen Yanmin. Clinical significance of serum PⅢNP, homocysteine, and hs-CRP/prealbumin ratio in patients with chronic heart failure complicated by pleural effusion [J]. Journal of Tuberculosis and Lung Disease, 2025, 6(3): 297-303. |
| [4] | Yang Shuqi, Li Feng. Advances in PD1/PD-L1 inhibitors in tuberculosis research [J]. Journal of Tuberculosis and Lung Disease, 2025, 6(1): 94-101. |
| [5] | Chen Yanling, Wu Di, Chen Xiuping, Lin Yujun, Chen Xiaohong. Study on the changes in lymphocyte subsets during secondary pulmonary tuberculosis dissemination and its clinical significance [J]. Journal of Tuberculosis and Lung Disease, 2024, 5(4): 294-304. |
| [6] | Chen Muxing, Fan Xinxin, Chen Xiaohong, Lin Youfei, Huang Mingxiang, Chen Lizhou, Wu Di. Research progress of the clinical value of applying T lymphocyte subsets examination in COVID-19 patients [J]. Journal of Tuberculosis and Lung Disease, 2022, 3(4): 343-346. |
| [7] | LI Yuan-yuan, SU Dong-dong, Aertai . Analysis of drug resistance characteristics and influencing factors in 159 patients with re-treated pulmonary tuberculosis [J]. Journal of Tuberculosis and Lung Disease, 2021, 2(4): 347-351. |
| [8] | SHEN Cong, JIAO Lei, BAI Lu, ZHANG Yi-li, GUO You-min. Analysis of the dynamic evolution of Chest CT lesions quality and peripheral blood lymphocyte count in patients with coronavirus disease 2019 [J]. Journal of Tuberculosis and Lung Disease, 2020, 1(2): 126-130. |
| [9] | Zheng-hua ZHOU,Bao-jiang WEN,Sheng-hong GONG,Zhi-yong LIANG. The prognostic value of the combined detection of serum procalcitonin, hypersensitive c-reactive protein and d-dimer in patients with acute exacerbation of chronic obstructive pulmonary disease [J]. Journal of Tuberculosis and Lung Health, 2019, 8(4): 289-293. |
| [10] | ZHANG Hong-hui,HUANG Wei.. Clinical effect of inhaled budesonide suspension for the treatment of asthma in children [J]. Journal of Tuberculosis and Lung Health, 2019, 8(3): 188-191. |
| [11] | FAN Yin-mei, LIU Qun-qun, MIAO Yan-fang, TANG Shen-jie. Clinical significance of peripheral blood mononuclear cells in tuberculosis patients [J]. Journal of Tuberculosis and Lung Health, 2017, 6(3): 246-249. |
| [12] | LI De-xian*, ZHANG Tian-tuo, TAN Shou-yong. The role of IL-17 in immune response to tuberculosis [J]. Journal of Tuberculosis and Lung Health, 2014, 3(1): 60-63. |
| [13] | LUO Yong-qiang*, LIN Dong-zi, ZENG Jin-cheng. Detection of peripheral blood Th17 cell subsets and serum IL-17A and IL-23 in the patients with pulmonary tuberculosis [J]. Journal of Tuberculosis and Lung Health, 2014, 3(1): 21-24. |
| [14] | ZHU Hai-xing,ZHOU Ling,SHI Guo-chao,WANG Lin-lin,PAN Li-na,WAN Huan-ying. The prevalence of blood Thl7 and CD4+CD25+Treg cells in patients with non-small-cell lung cancer [J]. Journal of Tuberculosis and Lung Health, 2013, 2(2): 100-105. |
| Viewed | ||||||
|
Full text |
|
|||||
|
Abstract |
|
|||||
 京公安网备11010202008787号
Total visitors: Visitors of today: Now online:
京公安网备11010202008787号
Total visitors: Visitors of today: Now online:
 This work is licensed under Creative Commons Attribution 3.0 License.
This work is licensed under Creative Commons Attribution 3.0 License.