结核与肺部疾病杂志 ›› 2025, Vol. 6 ›› Issue (4): 432-435.doi: 10.19983/j.issn.2096-8493.20250043
柳静, 赵月娟( )
)
Liu Jing, Zhao Yuejuan()
摘要:
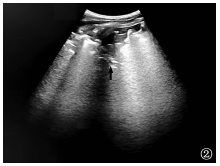
目的: 探讨高海拔环境下胸膜下肺结核与细菌性肺炎的超声影像学特征。方法: 采用回顾性研究方法,选取2024年1—12月云南省传染病医院确诊的47例胸膜下肺结核患者(肺结核组)及40例细菌性肺炎患者(肺炎组)作为研究对象。所有患者均接受常规超声检查,比较两组病灶形态(楔形、类圆形、不规则形)、碎片征(局部回声不均伴散在强光点)、瀑布征(层状无回声区与胸膜线平行延伸,记录其延伸范围及层状结构的清晰度)、液化坏死灶(无回声区内部可见气体强回声或“彗尾征”)等超声影像学特征。结果: 肺结核组中,楔形病灶占61.7%(29/47),类圆形病灶占29.8%(14/47),不规则形病灶占8.5%(4/47);肺炎组中,楔形病灶占62.5%(25/40),类圆形病灶占37.5%(15/40),两组在病灶形态分布上比较,差异无统计学意义(Fisher精确概率法,P>0.05)。肺结核组出现碎片征者占29.8%(14/47),明显低于肺炎组的82.5%(33/40),差异有统计学意义(χ2=14.490,P=0.001)。肺结核组出现“瀑布征”者占61.7%(29/47),明显高于肺炎组的27.5%(11/40),差异有统计学意义(χ2=10.177,P=0.001)。肺结核组出现液化坏死灶者占80.9%(38/47),明显高于肺炎组的25.0%(10/40),差异有统计学意义(χ2=28.301,P=0.001)。肺结核组有周边血流信号者占68.1%(32/47),有中央型血流者0例;肺炎组有周边血流信号者占77.5%(31/40),有中央型血流者占2.5%(1/40),差异无统计学意义(χ2=0.976,P=0.317)。结论: 高海拔环境下肺结核超声影像以层状无回声(瀑布征)伴气体强回声为特征,而细菌性肺炎以碎片征及小片液化灶为主,血流信号均以周边分布为主。
中图分类号:
 京公安网备11010202008787号
ip访问总数: ip当日访问总数: 当前在线人数:
京公安网备11010202008787号
ip访问总数: ip当日访问总数: 当前在线人数:
 本作品遵循Creative Commons Attribution 3.0 License授权许可
本作品遵循Creative Commons Attribution 3.0 License授权许可